Understanding Sternoclavicular (SC) Joint Instability
The shoulder complex is made up of several joints that work together to give your arm its incredible range of motion. While most people are familiar with the main ball-and-socket joint, there are other, smaller joints that are just as crucial for function and stability. One of these is the sternoclavicular (SC) joint, and when it becomes injured, it can lead to a rare but potentially serious condition known as sternoclavicular joint instability.
SC joint instability occurs when the ligaments connecting your collarbone (clavicle) to your breastbone (sternum) are stretched or torn, causing the joint to become loose or dislocate. Because this joint is the primary connection between your arm and the main part of your skeleton, an injury here can be both painful and alarming.
This article will provide a detailed, patient-friendly guide to understanding SC joint instability. We will explore what the SC joint is, the powerful forces required to injure it, the different types of dislocations, the symptoms to watch for, and how doctors diagnose this uncommon condition.
What is the Sternoclavicular (SC) Joint?
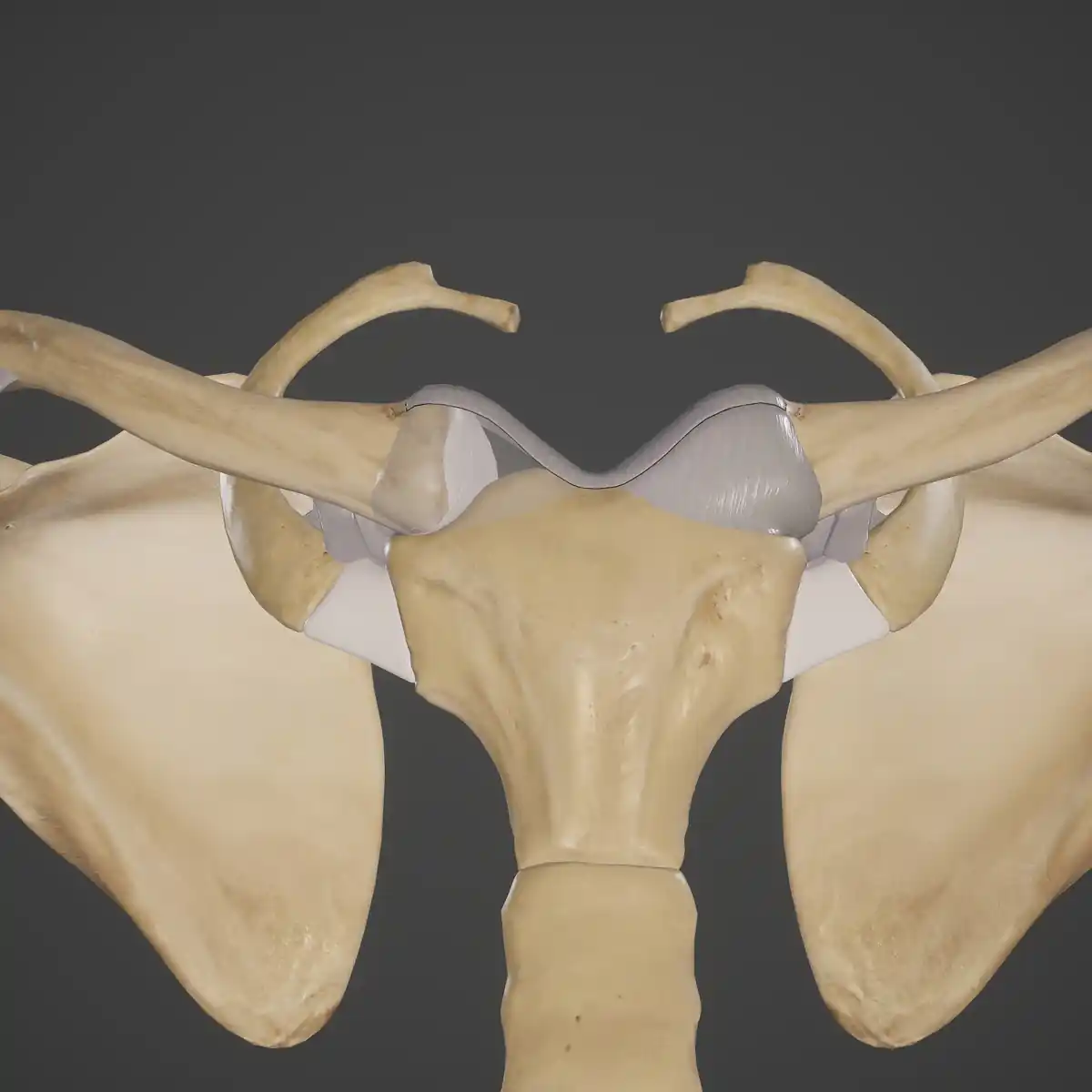
The sternoclavicular joint is the small but mighty joint located right where your collarbone meets the top of your breastbone, at the base of your neck. You can feel it as the bony prominence on either side of the small notch at the bottom of your throat. Though small, this joint plays a huge role in shoulder function, allowing you to lift your arm, reach overhead, and shrug your shoulders.
The SC joint is exceptionally stable. It is reinforced by some of the strongest ligaments in the body, which anchor the collarbone firmly to the breastbone. This robust design means that it takes a tremendous amount of force to injure the SC joint. Unlike the main shoulder joint, which is prone to dislocation, the SC joint is incredibly resilient. In fact, it is more common for the collarbone itself to break than for the SC joint to dislocate. When it does become unstable, it is almost always the result of significant trauma.
How Does Sternoclavicular Joint Instability Occur?
SC joint instability is rare precisely because the joint is so strong. Injuries almost always result from a high-impact event that transmits a powerful force directly or indirectly to the joint.
Common causes include:
- Motor Vehicle Accidents: This is one of the most frequent causes. An impact from a collision, such as a person's chest hitting the steering wheel or dashboard, can generate enough force to disrupt the joint.
- Contact Sports: A hard fall or a direct blow during sports like football, rugby, or hockey can lead to an SC joint injury. This might happen from a player being piled on or taking a direct hit to the collarbone area.
- Falls: Falling hard onto your side can create a compressive force that travels through the shoulder and into the SC joint, causing it to fail.
The force of the impact determines the direction in which the joint dislocates. This is a critical distinction, as the direction of dislocation has major implications for the seriousness of the injury.
Types of SC Joint Dislocations: Anterior vs. Posterior
When the SC joint dislocates, the inner end of the collarbone can be pushed either forward or backward relative to the breastbone.
Anterior Dislocation
This is the more common type of SC joint dislocation. In an anterior dislocation, the end of the collarbone is pushed forward, coming to rest in front of the breastbone.
- Appearance: This typically creates a very noticeable, hard lump at the base of the neck, right over the joint.
- Severity: While painful and visually alarming, an anterior dislocation is generally less dangerous because the displaced bone moves away from the critical structures located behind the breastbone.
Posterior Dislocation
This type of dislocation is much rarer but is considered a medical emergency. In a posterior dislocation, the end of the collarbone is forced backward, behind the breastbone and into the upper chest cavity (the mediastinum).
- Appearance: There may not be an obvious bump. In fact, the area might look sunken in.
- Severity: This is a life-threatening injury. The displaced end of the collarbone can press on vital organs and structures located in the upper chest, including:
- The trachea (windpipe)
- The esophagus (swallowing tube)
- Major blood vessels like the aorta and subclavian arter
Pressure on these structures can cause severe breathing difficulties, circulatory problems, and other catastrophic issues. For this reason, a suspected posterior SC joint dislocation requires immediate emergency medical attention.
Sprains and Subluxations
Not all SC joint injuries are complete dislocations. It's also possible to have a sprain, where the ligaments are stretched but not completely torn, or a subluxation, where the joint partially slips out of place and then goes back in. These are less severe but can still be painful and may lead to a feeling of chronic looseness in the joint, especially in individuals with naturally hypermobile or "loose-jointed" ligaments. Some people with generalized laxity might notice a painless "pop" or slip at the SC joint with certain movements, which is a form of minor, atraumatic instability.
Signs and Symptoms of an SC Joint Injury
The symptoms of SC joint instability will vary depending on the severity and type of injury.
For all SC joint injuries, you may experience:
- Pain: The most common symptom is pain localized directly over the SC joint at the base of the neck. The pain usually worsens with any movement of the arm, especially lifting it overhead or reaching across the body.
- Swelling and Bruising: The area over the joint will likely become swollen, tender, and bruised.
- Limited Arm Motion: Due to pain, you will likely find it difficult to move your arm and shoulder.
- Popping or Grinding: You may feel or hear a popping, clicking, or grinding sensation (crepitus) when you try to move your arm, as the unstable joint surfaces move against each other.
Specific signs of an anterior dislocation:
- A Visible Lump: A prominent, hard bump will be visible and palpable over the SC joint. This is the end of the collarbone sticking forward.
Emergency signs of a posterior dislocation:
A posterior dislocation is a life-or-death emergency. If you experience any of the following symptoms after a major trauma, seek help immediately:
- Difficulty Breathing or Shortness of Breath
- A Choking Sensation or a Hoarse Voice
- Difficulty Swallowing
- A Feeling of Fullness or Pressure in the Throat
- Numbness, Tingling, or Discoloration in the Arm (indicating pressure on blood vessels or nerves)
These are red-flag symptoms that suggest the dislocated collarbone is compressing vital structures in the chest.
Diagnosing Sternoclavicular Joint Instability
Because SC joint injuries are rare, a careful and thorough evaluation by a medical professional, often an orthopedic specialist, is essential.
- Medical History and Physical Exam: The doctor will start by asking how the injury occurred, looking for a history of high-impact trauma. They will then carefully examine the area, looking for the telltale bump of an anterior dislocation or the more subtle signs of a posterior one. They will assess your arm's range of motion and check for any signs of breathing or circulatory problems.
- Imaging Studies: Standard X-rays of the SC joint can be difficult to interpret because of the other bones of the chest that overlap in the image. While they may be taken, they often don't provide a clear view of the joint's alignment.
- Computed Tomography (CT) Scan: A CT scan is the gold standard for diagnosing an SC joint dislocation. It provides a detailed, cross-sectional view of the joint and surrounding structures, allowing the doctor to clearly see the position of the collarbone and determine if it is displaced anteriorly or posteriorly. A CT scan can also identify any associated fractures.
The Impact of an SC Joint Injury on Daily Life
After an SC joint injury, the recovery and impact on your life will depend on the severity.
For a mild sprain or a managed anterior dislocation, the initial phase involves pain control and immobilization. You will likely wear a sling or a special figure-of-eight brace for several weeks to keep the arm and shoulder still, allowing the ligaments to heal. During this time, daily activities will be challenging. Simple tasks like dressing, writing, or lifting objects will be difficult and painful.
After the period of immobilization, a program of gentle rehabilitation is usually started to gradually restore motion and strength to the shoulder. Most people with sprains and anterior dislocations can expect to make a good recovery over time, returning to their normal activities without long-term functional problems. Even if a visible bump from an anterior dislocation remains, it often becomes a cosmetic issue that does not affect how the shoulder works.
For a posterior dislocation, the immediate priority is emergency medical treatment to reduce the joint and relieve any pressure on the vital structures in the chest. The recovery after a successful reduction is similar to that of an anterior dislocation, involving immobilization and rehabilitation.
In a small number of cases, the SC joint may remain chronically unstable or painful. This can be frustrating, as any movement of the arm can cause a painful click or slip at the joint. This might limit a person's ability to participate in sports, perform heavy labor, or engage in overhead activities.
Conclusion
Sternoclavicular joint instability is a rare but significant injury that occurs when the strong ligaments connecting the collarbone to the breastbone are damaged. It is almost always caused by high-impact trauma. While an anterior dislocation is more common and less dangerous, a posterior dislocation is a true medical emergency that requires immediate attention due to the risk of life-threatening complications.
If you have sustained a major injury and have pain, swelling, or a deformity at the base of your neck where the collarbone meets the chest, it is crucial to be evaluated by a medical professional right away. An accurate diagnosis, especially with a CT scan, is key to understanding the nature of the injury.
The good news is that with proper medical care, most people with SC joint injuries can achieve a good recovery. Whether through immobilization and rehabilitation for less severe injuries or emergency intervention for posterior dislocations, the goal is to restore stability and allow you to return to a full and active life.
Frequently Asked Questions
Is an SC joint dislocation the same as a shoulder separation?
No. A shoulder separation is an injury to the acromioclavicular (AC) joint, at the outer end of the collarbone on top of the shoulder. An SC joint dislocation is an injury at the inner end of the collarbone, where it meets the breastbone in the center of your chest. They are two different injuries.
Why is a posterior SC joint dislocation so dangerous?
A posterior dislocation is dangerous because when the inner end of the collarbone is pushed backward, it can press on the vital structures in the upper chest, including the windpipe, esophagus, and major blood vessels. This compression can cause life-threatening breathing and circulation problems.
I have a bump near my collarbone after an injury. Will it go away?
If you have an anterior SC joint dislocation, the bump is the end of your collarbone that has popped forward. In many cases, even after treatment, this bump may remain. Fortunately, a persistent bump from an anterior dislocation is usually a cosmetic issue and does not typically cause long-term pain or functional problems.
Do all SC joint dislocations require surgery?
No. Many anterior dislocations and sprains can be managed successfully without surgery, using a sling for immobilization followed by physical therapy. Posterior dislocations require an emergency procedure to put the joint back in place, but this is often done without open surgery. Surgery is generally reserved for rare cases of chronic, painful instability that don't respond to other treatments or for dislocations that cannot be put back in place with manual techniques.
How can I tell if I have a posterior dislocation?
You cannot diagnose it yourself, but you should go to the emergency room immediately if, after a significant injury, you have pain at the SC joint plus any difficulty breathing, a hoarse voice, trouble swallowing, or a choking sensation. These are red-flag symptoms for a posterior dislocation.
I have very flexible joints and my SC joint sometimes pops. Is this a problem?
Some people with generalized hypermobility ("loose joints") can experience minor, painless popping or subluxation of their SC joint. If this is not painful and does not limit your activity, it is often not a major concern. However, if it happens frequently, becomes painful, or feels unstable, you should have it evaluated by a doctor.